

“We are trying to get the house of medicine back in order.” That’s how one emergency-department doctor describes his efforts to rethink his work amid the still-mounting opioid epidemic. The scale of the crisis is almost unimaginable—70,000 lives lost to overdose in 2017, of which 68 percent involved opioids; American lifespans contracting in part because of addiction; an estimated $1 trillion lost in economic output. But the origin story is somewhat clearer: overprescribing that began in the 1990s, sparked by a combination of aggressive marketing by pharmaceutical companies and doctors’ well-intentioned desire to address pain, a long-overlooked complaint. Nearly 30 years later, the problem has galloped beyond prescription pills to other opioids like heroin and fentanyl. As the country struggles toward countermeasures and solutions, Harvard-affiliated physicians and medical researchers turn to their own corners of the crisis—redefining addiction care, racing to find alternative drugs—working to help solve a problem that began, in part, in their own house.
When Addicts Reach the ER: A “Bridge Clinic”
Maybe it was the 2 a.m. phone calls he found himself making more and more, to tell the families of his patients that their son or daughter—age 25, age 19, age 30—had died. Or the growing number of overdoses he saw, knowing that even after he revived someone, there wasn’t much lasting help he could offer. Or the increasingly gnawing sense that some patients were using him for prescriptions, demanding opioids for every back pain, shoulder pain, and headache—and becoming confrontational whenever he hesitated. “About 10 years ago,” says Scott Weiner, M.P.H. ’04, an emergency physician at Brigham and Women’s Hospital, “I began to realize that the most frustrating, the most wrenching, part of my job was opioid-related issues.”
For most of his career, the standard emergency-department treatment for patients in withdrawal from opioids was temporary medication to level out their symptoms—something like clonidine or benzodiazepine, which can reduce anxiety, pain, and other discomforts—“and then we’d give them a piece of paper that had a list of detox facilities, and we’d say, ‘Good luck to you,’” he says. “That’s what is done in emergency departments across the country, day after day. Still.” For physicians accustomed to summoning cutting-edge, life-saving treatment for strokes, heart attacks, and other profound traumas, it was disempowering. “I think it fed into the stigma about patients with opioid addictions, honestly—because without anything to offer, you put that patient in a corner after an overdose, and you may not treat them as humanely.”
That’s changing now. In 2018, Brigham opened a “bridge clinic” to give temporary care to patients who come to the hospital with opioid-use disorder but cannot immediately enroll in long-term treatment. “It’s a low, low barrier to access” at the bridge clinic, Weiner says. “We’ll make you an appointment, but if you don’t get an appointment, that’s OK. We’ll still take care of you. If you relapse? That’s OK. We’ll still take care of you.” Doctors start patients on buprenorphine in the emergency department—a requirement of the Massachusetts opioid law enacted last summer—and continue care in the clinic. “Being able to give someone Suboxone”—a brand-name medication containing buprenorphine, which reduces opioid cravings and suppresses withdrawal symptoms—“means they don’t have this fear of withdrawal, they’re not desperately thinking about where they’re going to get their next dose of heroin. And then it’s like, everything normalizes and they can move forward.” So far it seems to be working: the clinic has treated roughly 200 patients since opening last April, and the retention rate, meaning patients who are still in treatment there or have transferred to a long-term facility, is 90 percent. “That’s extremely high.”
As president of the Massachusetts College of Emergency Physicians, Weiner lobbied the state to set up a prescription-monitoring program, a database where doctors can check patients’ other prescriptions—to see, for instance, whether they already have opioid prescriptions elsewhere. The resulting MassPAT was initiated in 2016, and within a year, 97 percent of the state’s opioid prescribers were using it. Weiner also chairs Brigham’s opioid-response and -education program, which coordinates services and guidelines across the hospital and its affiliated clinics. That work is informed by disturbing research findings: a 2015 study by Weiner and several coauthors that examined opiate prescriptions coming out of emergency departments from 19 different hospitals around the country. “And we found that 17 percent of all discharged patients were walking out of the emergency department with an opioid prescription,” he says. “People come in because they have a bellyache or gastritis or non-cardiac chest pain or a viral infection, and one in six of those patients was leaving with an opioid. There’s good research coming out now showing that in many cases, if you give someone ibuprofen, they do just as well after a couple of days as they do on hydrocodone. So why would you give them the drug that puts them at risk for long-term use?” Now, more than three years later, the number of patients discharged from Brigham’s emergency department with an opioid prescription is closer to 3 percent. Meanwhile, Weiner hopes to boost buprenorphine, by making sure every Brigham physician is certified to prescribe it; federal law requires an eight-hour training course and a waiver for certification, an encumbrance he wants to abolish. “In 2018, it makes no sense to add hurdles to treatment,” he says. “The ridiculous thing is, I can prescribe you 100 pills of Dilaudid”—a brand name of the opioid hydromorphone—“right now, without that training.”
More controversially, Weiner is working to widen access to naloxone, a medication used in emergencies to reverse an overdose, “to get it to people when they need it.” Naloxone is available over the counter in most states, including Massachusetts, but Weiner would like to see public-access stations set up, where someone could grab the medicine in an emergency. In a study last year, he found that 49 of 50 random bystanders were able to administer it effectively with no prior experience. He’s also working on a wearable device that senses oxygen saturation. “In an overdose, what happens is that your brain doesn’t tell your body to breathe, and then you suffocate.” The device would set off an alarm when the wearer’s oxygen fell too low, and then alert a designated friend or family member to come to the rescue. “There have been cases where someone is using in their bathroom at home, and their mother is in the kitchen, with no idea that her child is overdosing in the next room.”
Asked what keeps him up at night, Weiner pauses for a moment. “I’ll put it this way,” he says: “there are three buckets of patients I think about”: those who are already addicted and need care, those with chronic pain who seem to manage adequately on high-dose prescriptions, and then patients who have never taken opioids before. “The opioid-naïve,” Weiner says. “Those are the ones I worry about the most. How do we keep them safe?”
“A Crisis of Access”: Toward Policies That Work
Before he was a healthcare researcher knee-deep in data on what he calls “the largest, most poorly controlled public health emergency in the United States,” Michael Barnett, M.D. ’11, M.S. ’16, was a primary-care doctor. He saw patients every day as an internist at Brigham and at Faulkner Hospital in Jamaica Plain. That was when he first began to notice things, and to worry.
Physicians were aware, Barnett says, of the many and troubling challenges of caring for patients whose conditions sometimes overlapped in distressing ways: those with chronic pain, with long-term opioid therapy, and with addiction. Long before opioid-overdose deaths spiked upward, along with the public discussion, “It was clear there was a big problem here.” He saw it as a trainee: “There was just no evidence and no guidance about how to prescribe these medications. Like, when are opioids best indicated for certain kinds of pain? Which of the many different opioid formulations should we use? How many pills should we give? How do we know if the patient is failing therapy or not? All these questions.”

Many new laws aimed at opioids “feel like the right thing to do,” says researcher Michael Barnett, but not all are effective.
Photograph by Jim Harrison
Those questions pushed him into research. Still a practicing internist, he is also assistant professor of health policy and management at the Harvard T.H. Chan School of Public Health, where he received his master’s degree. Early on, like many researchers trying to make sense of the crisis, Barnett focused on physician prescribing practices, and the clinical knowledge—or lack thereof—that undergirded them. “The evidence base for how to prescribe opioids, or really any pain medication, is very underdeveloped, compared to what we have in areas like cardiology or oncology,” he explains. He recalls the now-dismissed concept of “pseudoaddiction,” adopted into the mainstream two decades ago but never empirically verified; it argues that drug-seeking behavior in patients with chronic pain is not a sign of opioid-use disorder, but of under-treatment. “And so the solution was to increase their dosage,” Barnett says. “I was actually taught that concept in medical school, which was not that long ago, and I went to medical school at Harvard.”
In 2017, Barnett published a study in The New England Journal of Medicine (NEJM) that challenged, indirectly, the assumption on which the idea of pseudoaddiction rested: that the risk of addiction is negligible for patients truly in pain. He used data from hospital emergency departments between 2008 and 2011 (when the number of prescriptions was still increasing) to approximate a randomized experiment: patients do not choose their emergency physicians, and opioid-prescribing habits vary widely among those doctors. Barnett and his coauthors found that those patients treated by a “high-intensity” opioid prescriber were much more likely to transition into long-term opioid use. “Even a short opioid prescription that you get in the emergency room—because these doctors are not writing for 60 days of opioids, they’re writing for three, seven, maybe 14 days at the very most—carries a real risk of long-term use or dependence.” For every 49 prescriptions written, he found, one patient would wind up on opioids long term. “Which is substantial, given that opioids are among the top two or three most-prescribed medication classes. In some states, one-third to two-thirds of residents will receive an opioid prescription in any year.”
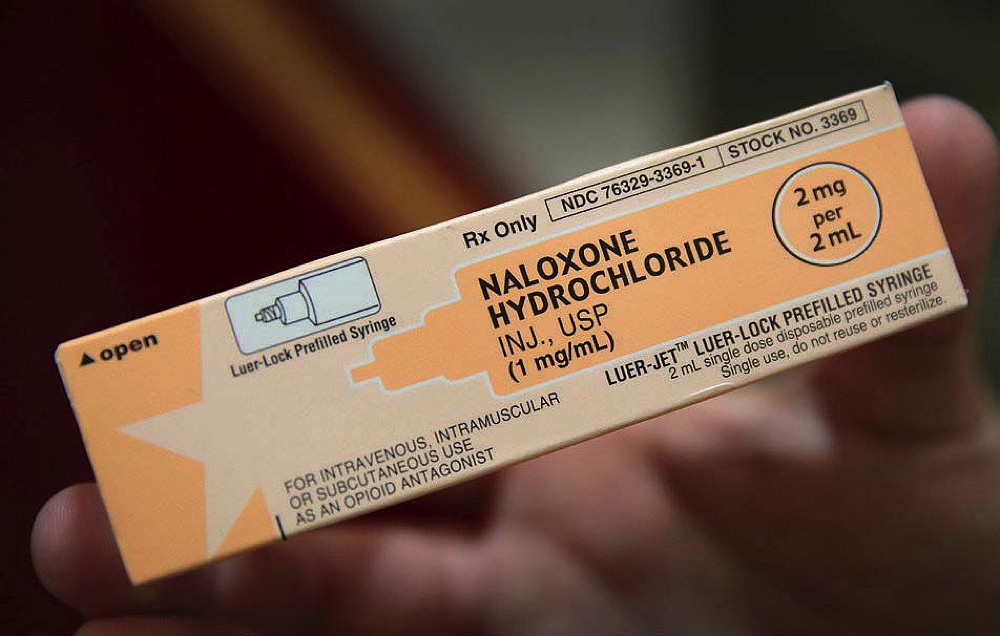

“We have effective treatments,” says Barnett: naloxone (top) rapidly reverses the effects of overdose; and buprenorphine (bottom), a component of long-term addiction therapy, curbs opioid cravings and withdrawal.
In other studies Barnett has looked into the flurry of state statutes passed amid the gathering crisis: regulations on pill mills, laws against doctor-shopping, restrictions on prescribing. Some states have launched prescription-drug monitoring programs, setting up databases like the one Weiner, the Brigham emergency physician, advocated for in Massachusetts, in which doctors can check the prescription histories of their patients. That measure seems to cut down on high-risk patterns, like patients shopping for doctors or using multiple pharmacies, Barnett says, but it hasn’t correlated strongly to lower rates of addiction or overdose. A policy recently adopted in Massachusetts—issuing letters to high-prescribing doctors comparing their prescription rates to those of their peers—produced no meaningful change in behavior that Barnett could find. “We can’t just pass these opioid laws because they feel like the right thing to do,” he says. “We actually have to have an outcome we’re looking to change, and build some type of evaluation into the law.…If not, then why burden physicians with more forms and letters and regulations when they’re already overloaded?”
Lately, though, Barnett has shifted focus, toward treatment and the barriers to access. So much energy has already been poured into research and policy on opioid prescribing, and increasingly, he says, “the swing of the pendulum is from overprescribing opioids to being overly frightened of medications in terms of liability, legal exposure, and harming patients.” Moreover, the crisis has mutated beyond prescription opioids. Overdose deaths from the synthetic opioid fentanyl—a painkiller-turned-street-drug—have been escalating every year, and now outstrip those from prescription pills and even heroin. In December, the Centers for Disease Control declared fentanyl America’s deadliest drug, responsible for more than 18,000 overdose deaths in 2016, or 29 percent of the total.
“We have an epidemic on our hands, accelerating year after year, and for me now the question is, how can we stop it?” Barnett asks. “Until treatment is as easy to access as heroin or fentanyl, we can’t really expect to make a dent in this. There’s a population of people out there who, through their genetics and their environment, are going to develop opioid-use disorder. We’re not going to make addiction disappear.” Instead, he says, more primary-care doctors should prescribe buprenorphine. That was the core argument of a 2018 paper he published in NEJM with Massachusetts General Hospital (MGH) addiction-medicine physician Sarah Wakeman, an assistant professor of medicine. “None of us can say, ‘Somebody else is going to deal with this,’” Barnett says. “No one says, ‘Well, the cardiologist will deal with high blood pressure,’ or ‘The endocrinologist will deal with diabetes.’ There’s no physician out there who would see a patient with uncontrolled, untreated diabetes and then just send them back into the community without any guidance.”
“We have an epidemic on our hands, accelerating year after year…. Until treatment is as easy to access as heroin or fentanyl, we can’t really expect to make a dent in this.”
In ongoing research, Barnett looked at the barriers to access for buprenorphine, gathering data from several hundred clinics in areas of the country hardest hit by the crisis. At first, he expected long wait times and full doctor schedules to be the biggest issue; instead, he found, “It’s finding someone who is willing to prescribe you buprenorphine.” Even among doctors who complete the training required to prescribe it, there is tremendous reluctance to do so. They change their minds, or fear attracting patients they view as unreliable, or whom they judge likely to misuse or sell the medication. Some clinics lack the right setup to make it financially feasible to prescribe. “There’s a lot of stigma, and a lot of myth”—and a lot of missing infrastructure. Barnett elaborates: “If you get in a car accident in the middle of nowhere in Texas, someone can call 911, and after the emergency services extract you from your car, a helicopter will take you to a level-three trauma center within minutes.” Similar resources and procedures are standard for many other medical emergencies, but for opioid addiction, “It’s very hard to even find someone who accepts your insurance.”
“In some ways,” he sums up, “the opioid crisis is a crisis of access.”
Treatment Failure, Not Patient Failure
“Most people get better,” says MGH internist Sarah Wakeman. “That’s what we don’t ever talk about.” She describes opioid addiction as a chronic illness, but a treatable one. “There are 24 million people in this country living in long-term recovery. But often they’re not telling you they’re in long term recovery, because of the stigma of sharing that story.” Among the wider public, there is a sense that opioid addiction is a hopeless condition, that no one with the disorder will ever really get well, that they’ll always struggle, or they’ll die from their addiction. “But with treatment,” Wakeman says—medically assisted treatment, lasting for years, and sometimes for life—“most people do get well. And that’s what makes it so tragic when someone dies from an overdose, because it really never should have happened. We have medications to reverse the acute effects of an overdose”—naloxone, which can be injected or sprayed into the nose—“and then we have treatment for the underlying disease”—buprenorphine, one cornerstone of medically assisted treatment.
Wakeman is medical director of MGH’s substance-use disorder initiative. Its major component is a bridge clinic, opened in 2017—the first in Massachusetts—to serve as a temporary outpatient facility for people who arrive at the hospital’s emergency department with addiction, withdrawal, or overdose. Wakeman also maintains a practice in Charlestown, where she serves simultaneously as a primary-care and addiction-medicine physician. “Addiction medicine is very rewarding work,” she says, “which I think people don’t realize. Half my trainees say, ‘God, this must be so depressing, to do what you do.’ But patients get better, and often you get to play a role in people’s lives when they feel terribly alone.”
“Addiction medicine is very rewarding work, which I think people don’t realize....Patients get better, and often you play a role in people’s lives when they feel terribly alone.”
Wakeman can stick it out with patients through circumstances that often fracture relationships with loved ones. “As their doctor, I can solely care about what’s going to improve their health and quality of life. I can take care of them no matter what. If they want to continue to use heroin, I’ll still be their doctor.”
That was the case with Nicholas, a patient who came to MGH seven years ago for help, after an addiction that began with a back injury and a Percocet prescription. “I was instantly addicted,” he says. “I’d have some Percocets at six in the morning and wash it down with a beer.” This was in 2009, and Nicholas, who worked as a quality-control manager for a pharmaceutical company (though in cancer drugs, not pain medicines)—was living in New Hampshire. He had a wife and three children, and a home. “I was employee of the year twice.” A year later, all that was gone. His addiction shifted from the pills he’d been prescribed to the OxyContin a friend introduced him to, and, when he could no longer afford $50 per pill, to heroin. By 2010 he was jobless and intermittently homeless. And his diabetes was going unchecked. More than once, he’d come to the hospital to ask for help getting his blood glucose level under control and to get patched up so he could return to the street. Once, when staying at a friend’s house, he nearly died from lack of insulin. “My body started shutting down, and I woke up in the ICU, where they told me I’d had a cardiac breakdown. A heart attack, basically.”

Police in Philadelphia use Narcan to revive a man who overdosed on heroin. Since 2010, heroin use across the country has more than doubled.
Photograph by Spencer Platt/Getty Images
That scared him. Not long after, he came back to MGH, looking for help with his diabetes—and with his addiction. He remembers the moment Wakeman appeared at his bedside. “The sun was behind her, and she looked like an angel coming in,” he says. “And she said, ‘We have something that will help you.’” That something was Suboxone. “And I wanted it bad.”
But it wasn’t a straight road. For several years, Nicholas relapsed often, struggling to piece together more than brief stretches of sobriety. He was taking Suboxone, but he was also sometimes selling it. He was on and off heroin. He was in and out of homelessness. But he kept at it, starting antidepressants and mental-health counseling to supplement his addiction treatments. Wakeman stuck with him, and even when he was using, he kept his appointments with her, sometimes weekly, sometimes more often than that. Eventually he reached more solid ground. “I turned 50 this past June, and I’ve been clean since two months before that,” Nicholas said in October. Now he’s making plans for graduate school, and for a return to a career in science. He wants to be a researcher on addictions.
Caring well for people like Nicholas, Wakeman says, requires a different conceptual framework from the way most Americans think about addiction and recovery, a different kind of tenacity and flexibility. “Many people have this notion that you go to rehab to get better—and that would be wonderful, if you could go away for 30 days and be fixed,” she says. “But for most people, opioid addiction really is a chronic illness. Just like we don’t give you 30 days of diabetes treatment and then send you on your way,” addiction treatment takes time, a combination of medications plus counseling and behavioral change, and support. There is trial and error. Sometimes, especially in the beginning, patients go back to using and have to start over again. “You follow someone long term.…It’s a huge frame shift in how we think about caring for people.” To get better, patients must be allowed to return to treatment after relapsing, Wakeman says. “That’s one of the ways in which the system currently fails people. We continue to blame the person for failing. It’s very convenient to say, ‘He failed treatment.’ We talk about people failing drug tests. We use that language a lot—and yet we don’t blame people when chemotherapy doesn’t work. We talk about treatment failure. We talk about the need for different chemotherapy regimens.”
Wakeman went to medical school intending to become an HIV doctor. “That was the sexy thing for medical students—HIV and global health.” But during the summer after her first year, she did an internship at an HIV clinic in a state prison in Rhode Island. “I didn’t know much about prisons then, and basically everyone I met there had an addiction, everyone had trauma.” Nearly half of those in federal prison are serving time for drug offenses, but adding in crimes people commit to pay for drugs—theft, robbery, prostitution—pushes the number higher, Wakeman says. “That broke open my notions of what we imprison people for, and what addiction is.” Her path shifted.
Prisons remain an important segment of her practice—she runs a post-release clinic for people coming out of incarceration, who are at an elevated risk for fatal overdose. “It’s 130 times higher than the general population,” she says. “We are seeing people die at astonishing rates.” Last August, Massachusetts governor Charlie Baker ’79, a former health-insurance CEO, signed opioid legislation that included a pilot program to provide medically assisted treatment for opioid addiction in five state prisons—an essential step, Wakeman says, in curbing the crisis.
The fundamental principles of her approaches to treatment—multiple second chances for people struggling to break addiction, a care- rather than punishment-oriented outlook, and harm-reduction measures like clean injection sites and wide distribution of Narcan—are based on the sheer urgency of opioid addiction. Alcohol addiction still kills more people than opioids do (88,000 in 2017, according to the National Institutes of Health, versus 70,000 opioid overdose deaths), but that “takes years and often decades,” she says. There is more time to intervene. “Opioid addiction is imminently fatal.” That’s especially true after the widespread introduction of fentanyl, 50 times more potent than heroin. “For someone who’s actively using intravenous heroin or fentanyl, literally every day is a day that they could die. The stakes are very high.“
Combatting “Spontaneous Pain”: The Search for Opioid Alternatives
“The reality is, until there is a pain treatment as effective as an opioid, it’s going to be difficult to persuade patients and physicians.” That’s the crux for neurobiologist Clifford Woolf, one of the many scientists searching for safer, non-addictive alternatives to opioids. “Unless it’s as good or better at relieving pain, they won’t use it.”
“The reality is, until there is a pain treatment as effective as an opioid, it’s going to be difficult to persuade patients and physicians.”
And so he has been pushing. Woolf, professor of neurology and director of the Kirby Neurobiology Center at Boston Children’s Hospital, and Winthrop professor of neurobiology Bruce Bean have been inching for the past dozen years toward a drug that could replace opioids in treating acute postoperative pain (“spontaneous pain,” Woolf calls it, distinct from chronic pain). The pair have found several therapeutic compounds they believe could work, and continue to screen for others. Says Woolf, “We’ve got a set of leads that look very promising.”
Years ago, Woolf’s research revealed that the neurons that initiate pain signals are separate from other neurons, and have different receptors. One of those receptors is TRPV1, an ion channel that responds to painful heat and—importantly—has very large pores that span the membrane of the nerve cell. “What we realized,” Bean says, “is that these channels will admit very large, positively charged molecules.” Normally that means sodium ions, but Bean and Woolf wondered if they could make a charged version of a local anesthetic that would pass through these large pores and inhibit the electrical signaling of the pain-sensing nerve cells, leaving other neurons (like those that control motor function and the sympathetic nervous system) unhindered. “Because it’s targeted, it’s quite unlike a standard lidocaine injection at the dentist, where you feel numb and your mouth is paralyzed and you drool,” Woolf explains. “With this, you’d just inject into a particular tooth, and you wouldn’t feel anything, other than you won’t feel pain.”
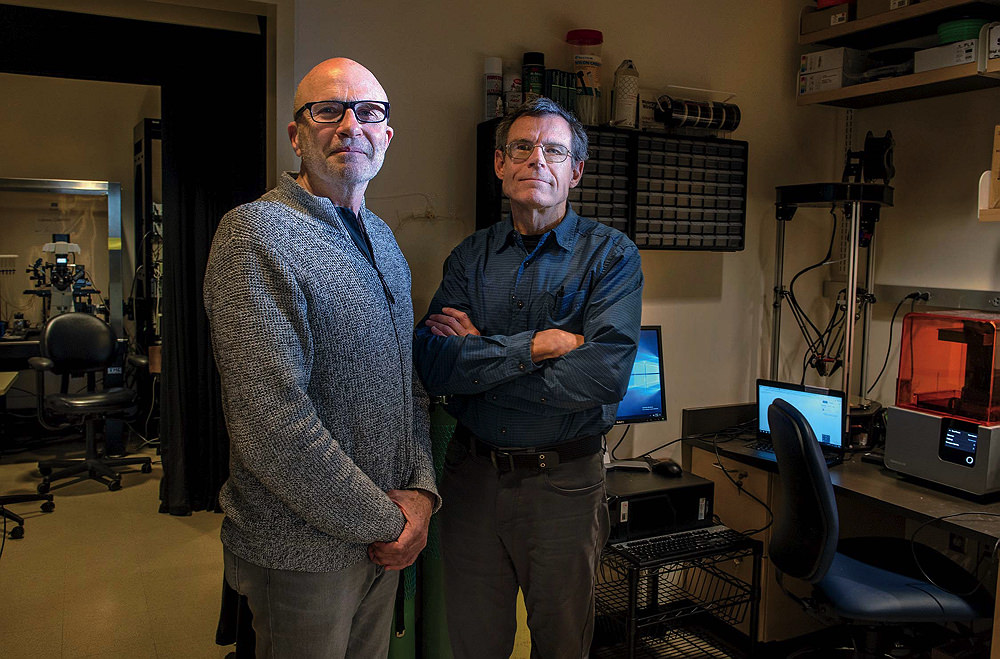
Clifford Woolf (left) and Bruce Bean are working to develop a new drug to treat post-surgical pain, which would allow many patients to skip opioids altogether.
Photograph by Jim Harrison
This treatment would work best for pain from an injury, or after surgery. Because the compound tends to remain in the nerve cell for 24 hours or more, Bean says, it could help patients cross an important threshold: “If this were given in the wound during surgery, it could probably tide the patient over during the night, when the pain is most intense, where you might otherwise give an oxycodone or something similar to blunt the initial pain.” Afterward, when the intensity—and the drug—subside, ibuprofen or acetaminophen should usually be enough, circumventing opioids altogether. “And that’s extremely important,” Bean adds, “because for a lot of people with opioid addiction, that’s where it all starts”—with a prescription after an operation. Woolf recalls his 15-year-old son coming home from a wisdom-tooth extraction several years ago with a prescription for 20 oxycodone. “To give that much to a teenager is unbelievable!” Bean remembers the oxycodone his wife was given immediately after ankle surgery, and how the supply far outlasted her need for it.
For Woolf especially, the study of pain is a lifelong preoccupation. He began working seriously to unwind its complexities when he was a medical student in South Africa during the early 1970s. The treatment for postoperative pain then was minimal. Woolf remembers walking through the surgical wards for the first time, and hearing patients cry out in anguish. “Absolutely miserable,” he says. But the surgeon answered his worry and shock with a shrug: “He said, ‘What do you expect? They’ve just had surgery.’” When Woolf asked if there was something they could do for them, the answer was no. “And so I started working right then.”
His research was the first to describe a phenomenon called “central sensitization,” in which the nervous system amplifies and perpetuates pain, becoming hypersensitive even to ordinary touch after prolonged exposure to harmful stimulus. Woolf showed that the nervous system is plastic, that pain can change its architecture and behavior. He has uncovered contributing factors to inflammatory pain, and the genetic components of pain-related disorders.

Needle-exchange programs allow drug users to trade in used syringes for clean ones, and can connect people to treatment, but remain controversial and are banned in many states.
Photograph by Carlos Giusti/AP Images
Then came the opioid crisis. By then Woolf and Bean were already collaborating on their new drugs, working to transform the flash of an idea they had one night in 2006 into a functioning compound. They published a paper in Nature on TPRV1 and its large pores in 2007. Then they began raising money (among the funders of their research is a grant from the Department of Defense, which sees a potential for mitigating acute pain from battlefield injuries without having to maintain large supplies of morphine), designing screens to identify compounds, and launching a biotech startup to bring their research to market. “We’ve pushed the translational envelope quite a lot further than typical,” Woolf says. “It wasn’t enough just to get a nice Nature paper and move on. We wanted this to work.”
Woolf is also investigating new ways to treat chronic pain, which works according to a different neural mechanism and would require a different drug. Long-term, neuropathic pain is less well understood, he says, and poorly medicated. He has begun using human stem cells with genetic predispositions to pain as a way to model pain and to design screens to search for a whole new set of compounds. Last September he coauthored a Nature paper identifying what Woolf called a “volume control” in the brain for pain—the pathway leading from the sensory cortex down the spine. “This is one of the loops that may drive the exaggeration of persistent pain,” he says. “Now we need to know how to turn it off.”








